The World Health Organization (WHO) describes non-communicable diseases (NCDs) as chronic ailments of the long term as a consequence of an interplay o …
Swasthya Pahal (Health for All): A Digital Health Intervention to Address Chronic NCDs
The World Health Organization (WHO) describes non-communicable diseases (NCDs) as chronic ailments of the long term as a consequence of an interplay of genetic, behavioral, physiological, and environmental factors.
India faces a huge burden of NCDs as it has undergone demographic and epidemiological shifts, leading to a transition from infectious diseases to NCDs. Consumption of tobacco and alcohol, sedentary lifestyle, overweight and obesity, increased intake of fat and sodium intake, and low intake of fruits and vegetables, are the various behavioral and biological risk factors of NCDs. Other factors such as individuals’ job profile and the workplace environment play a role in the development of NCDs. The WHO acknowledges the capability of digital health interventions for ensuring high-quality care to people. Information and Communication Technologies (ICTs) have the potential to offer affordable and high-quality services.
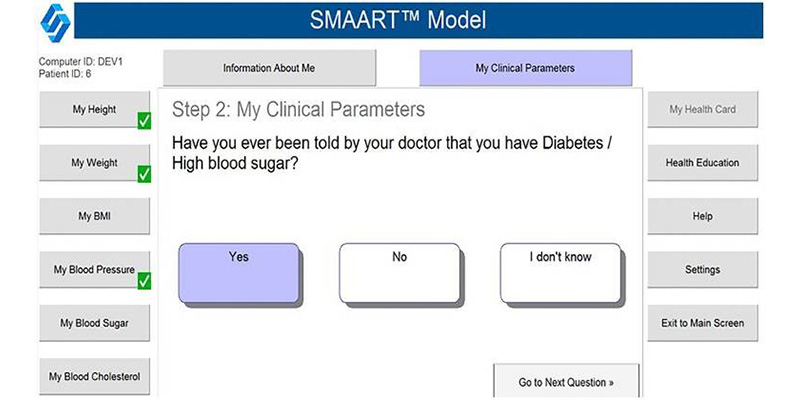
To address this rising burden of chronic NCDs, I discuss here one of our innovative digital health interventions, Swasthya Pahal (Health for All) (SP) launched in April 2012. Swasthya Pahal (Health for all) is an innovative community-based program, facilitated through an interactive, multi-lingual, standalone, and internet-enabled touch screen computer-based program that aims to enhance self-management of NCDs including diabetes, hypertension, and obesity among individuals living across diverse community settings.
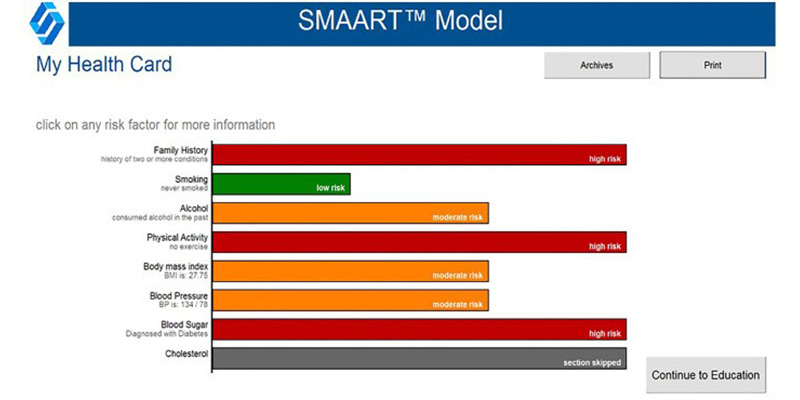
This community program facilitates the collection of individual subjective and objective data using the Population Health Informatics (PopHI) framework called SMAART (Sustainable Multisector Accessible Affordable Reimbursable Tailored). Data gathered includes subjective data and objective data.
Subjective data comprised responses to a sequence of multiple-choice questions, including (I) location of residence, (II) socio-demographic variables such as age (years), gender, the highest level of education attained (III) health behavior variables such as smoking, alcohol consumption, and physical activity patterns, (IV) clinical status assessments such as ever been told by a doctor about high blood sugar and high blood pressure and if currently being treated for their health conditions. Information related to Knowledge, Attitude, and Practices (KAP) about diabetes and hypertension self-management was also gathered. Objective data was collected using multiple physiological sensors which captured participants’ height, weight, blood sugar, and blood pressure levels. Algorithms (“if and then” rules applied to problem-solving) were applied to the garnered data to generate an electronic evidence-based report called a SMAART health card.
The program has been successfully implemented in diverse community settings including urban, urban slum, rural and geographically inaccessible settings such as hilly regions. The program has so far been covered in eight states of India over 400 health camps and screened more than 10,000 individuals across diverse geographic settings. In February 2016, we launched Swasthya Pahal initiative as a pilot program to address burden of chronic NCDs among police personnel of Delhi. Since then, more than 142 SP events have been conducted screening more than 5000 police personnel and providing them lifestyle intervention to support their good health and well-being. Nearly 75% of the Delhi police stations have been covered so far under this initiative. In 2018, the platform won the Digital Commonwealth Award. In 2020, we expanded the program to police personnel in the state of Uttarakhand.
Swasthya program implemented using the SMAART informatics framework can be utilized to screen obesity, diabetes, and hypertension for improved disease prevention, monitoring, and self-management of NCDs in a geographically inaccessible, underserved, under resourced environments in a cost-effective manner.
The next article will cover the cost of the Swasthya Pahal program implementation and program delivery. Contact Ashish Joshi for more information on Swasthya Pahal digital intervention.
With the creation of public health management cadre in the state, district, and block levels of India, there is a need for a comprehensive, synergisti …
The current state of public health education in India: A scoping review
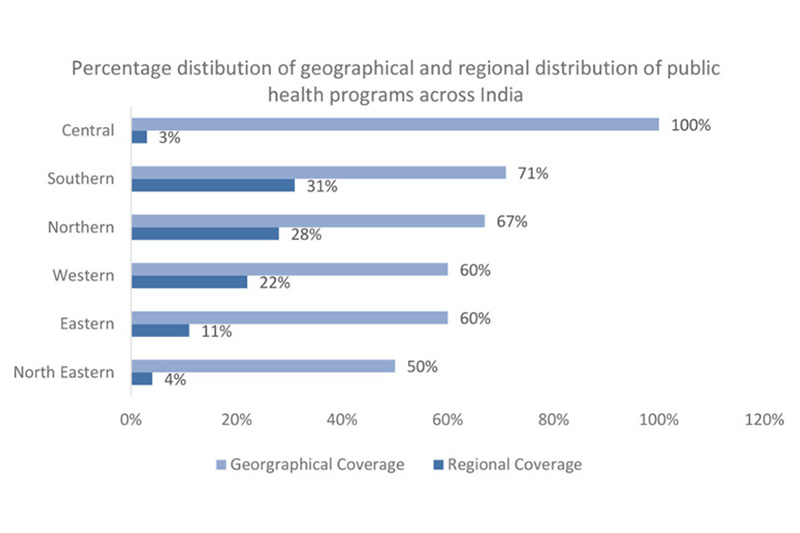
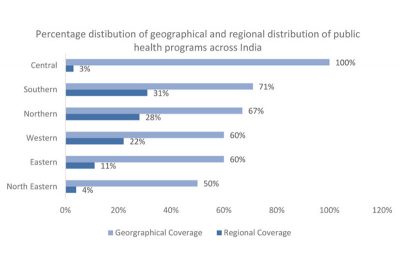 With the creation of public health management cadre in the state, district, and block levels of India, there is a need for a comprehensive, synergistic education system to ensure efficient public health across the country. This scoping review, therefore, aims to examine the characteristics of public health education programs available in India’s varied geographical and regional contexts. It examines 16 program-related descriptors across public health Doctoral, Masters, Bachelors, Post-graduate Diploma, and Diploma education programs offered. Data was retrieved through institutional websites. Results of our analysis showed 84 unique institutions in 20 states and 3 UTs currently offering 116 public health programs across India’s 28 states and 8 UTs. Private and public institutes were 65% (n = 75) and 35% (n = 41) respectfully. The majority of universities mainly provided Masters of Public Health (n = 73, 63%) programs followed by Postgraduate Diploma (PGD) and Diploma (n = 17, 15%), BPHSc (n = 14, 12%), and Ph.D. (n = 12, 10%). The majority of Ph.D. programs in public health are offered in Maharashtra, Karnataka, and Haryana, while Masters in Public Health programs are offered highest in Karnataka, Bachelors in Public Health programs in Rajasthan, Post Graduate Diploma in Public Health program in Delhi, and Tamil Nadu had the most number of Diploma in Public Health programs. Thirty-one percent (n = 36) of the public health programs are offered across the south, 28% (n = 32) across the north, and 22% (n = 26) across the west Analyzed descriptors provide comprehensive information on program characteristics, mainly admission, format, and tuition fee. The review offers five suggestions to improve collaborative public health education and prepare a workforce with the skills, knowledge, and expertise to respond to the twentyfirst century’s public health threats and challenges in India.
With the creation of public health management cadre in the state, district, and block levels of India, there is a need for a comprehensive, synergistic education system to ensure efficient public health across the country. This scoping review, therefore, aims to examine the characteristics of public health education programs available in India’s varied geographical and regional contexts. It examines 16 program-related descriptors across public health Doctoral, Masters, Bachelors, Post-graduate Diploma, and Diploma education programs offered. Data was retrieved through institutional websites. Results of our analysis showed 84 unique institutions in 20 states and 3 UTs currently offering 116 public health programs across India’s 28 states and 8 UTs. Private and public institutes were 65% (n = 75) and 35% (n = 41) respectfully. The majority of universities mainly provided Masters of Public Health (n = 73, 63%) programs followed by Postgraduate Diploma (PGD) and Diploma (n = 17, 15%), BPHSc (n = 14, 12%), and Ph.D. (n = 12, 10%). The majority of Ph.D. programs in public health are offered in Maharashtra, Karnataka, and Haryana, while Masters in Public Health programs are offered highest in Karnataka, Bachelors in Public Health programs in Rajasthan, Post Graduate Diploma in Public Health program in Delhi, and Tamil Nadu had the most number of Diploma in Public Health programs. Thirty-one percent (n = 36) of the public health programs are offered across the south, 28% (n = 32) across the north, and 22% (n = 26) across the west Analyzed descriptors provide comprehensive information on program characteristics, mainly admission, format, and tuition fee. The review offers five suggestions to improve collaborative public health education and prepare a workforce with the skills, knowledge, and expertise to respond to the twentyfirst century’s public health threats and challenges in India.
With the increasing global burden of dyslipidemia over the past 30 years, it is estimated that more than 200 million people worldwide are under statin …
A Scoping Review on the Reported Evidence and Gaps of the Risk of Diabetes in Dyslipidemic Patients under Statin Therapy
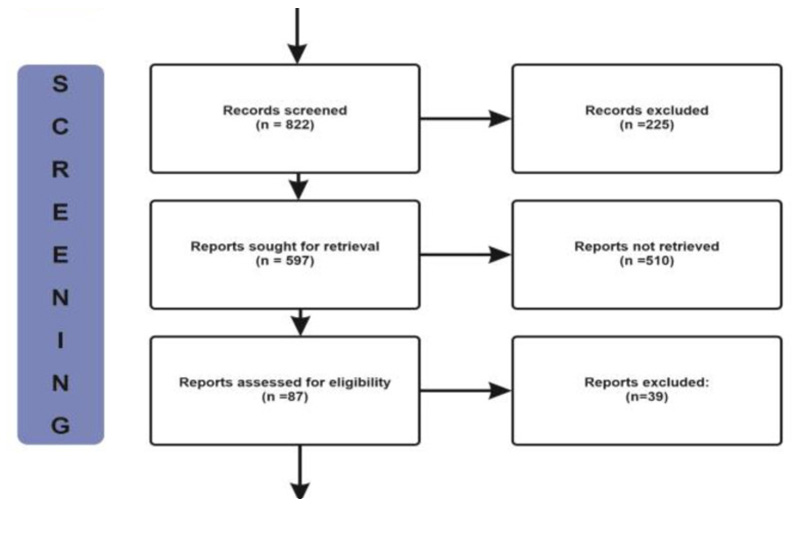
 With the increasing global burden of dyslipidemia over the past 30 years, it is estimated that more than 200 million people worldwide are under statin therapy. In India, roughly 25-30% of urban populations and 15-20% of rural populations have abnormal lipid levels. Statin, which is deemed to be the gold standard lipid-lowering agent, is the first treatment of choice for these patients. Although statins at one end are highly effective against dyslipidemiaand cardiovascular diseases, at the other end, they cause adverse effects including an increased risk of diabetes mellitus. The objective of this study was to understand the coexistence of diabetes and dyslipidemia in patients undergoing statin therapy. A scoping review was conducted with published articles selected from PubMed and Google Scholar. The obtained results were filtered based on inclusion/exclusion criteria. Our database search provided a total of 822 articles, of which 48 were selected for this review, with results concluding that statin users are potentially at a greater risk of developing diabetes mellitus compared with patients who are not using statins. Although many studies have been conducted to ascertain the onset of diabetes mellitus amongst statin users, the exact mechanism is not yet precisely established. Future studies are essential for identifying the exact cause of diabetes mellitus in statin users.
With the increasing global burden of dyslipidemia over the past 30 years, it is estimated that more than 200 million people worldwide are under statin therapy. In India, roughly 25-30% of urban populations and 15-20% of rural populations have abnormal lipid levels. Statin, which is deemed to be the gold standard lipid-lowering agent, is the first treatment of choice for these patients. Although statins at one end are highly effective against dyslipidemiaand cardiovascular diseases, at the other end, they cause adverse effects including an increased risk of diabetes mellitus. The objective of this study was to understand the coexistence of diabetes and dyslipidemia in patients undergoing statin therapy. A scoping review was conducted with published articles selected from PubMed and Google Scholar. The obtained results were filtered based on inclusion/exclusion criteria. Our database search provided a total of 822 articles, of which 48 were selected for this review, with results concluding that statin users are potentially at a greater risk of developing diabetes mellitus compared with patients who are not using statins. Although many studies have been conducted to ascertain the onset of diabetes mellitus amongst statin users, the exact mechanism is not yet precisely established. Future studies are essential for identifying the exact cause of diabetes mellitus in statin users.
The COVID-19 pandemic has underlined the need to partner with the community in pandemic preparedness and response in order to enable trust-building am …
A call for citizen science in pandemic preparedness and response: beyond data collection
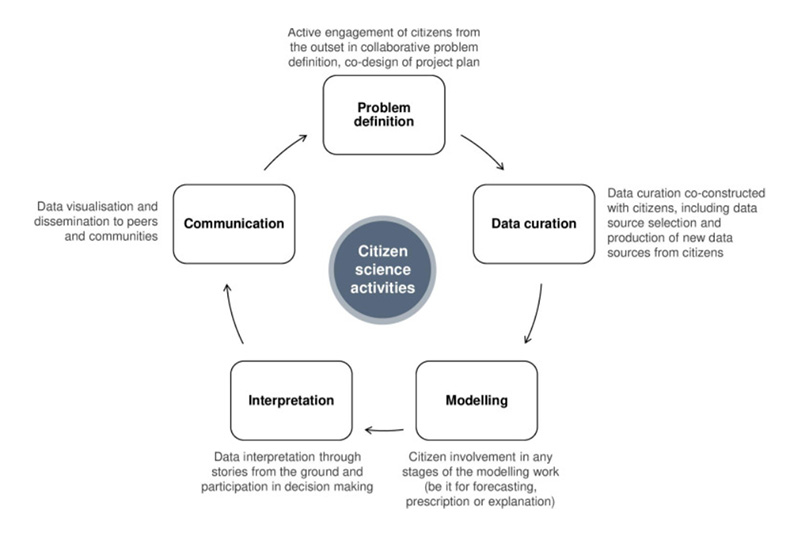
 The COVID-19 pandemic has underlined the need to partner with the community in pandemic preparedness and response in order to enable trust-building among stakeholders, which is key in pandemic management. Citizen science, defined here as a practice of public participation and collaboration in all aspects of scientific research to increase knowledge and build trust with governments and researchers, is a crucial approach to promoting community engagement. By harnessing the potential of digitally enabled citizen science, one could translate data into accessible, comprehensible and actionable outputs at the population level. The application of citizen science in health has grown over the years, but most of these approaches remain at the level of participatory data collection. This narrative review examines citizen science approaches in participatory data generation, modelling and visualisation, and calls for truly participatory and co-creation approaches across all domains of pandemic preparedness and response. Further research is needed to identify approaches that optimally generate short-term and long-term value for communities participating in population health. Feasible, sustainable and contextualised citizen science approaches that meaningfully engage affected communities for the long-term will need to be inclusive of all populations and their cultures, comprehensive of all domains, digitally enabled and viewed as a key component to allow trust-building among the stakeholders. The impact of COVID-19 on people’s lives has created an opportune time to advance people’s agency in science, particularly in pandemic preparedness and response.
The COVID-19 pandemic has underlined the need to partner with the community in pandemic preparedness and response in order to enable trust-building among stakeholders, which is key in pandemic management. Citizen science, defined here as a practice of public participation and collaboration in all aspects of scientific research to increase knowledge and build trust with governments and researchers, is a crucial approach to promoting community engagement. By harnessing the potential of digitally enabled citizen science, one could translate data into accessible, comprehensible and actionable outputs at the population level. The application of citizen science in health has grown over the years, but most of these approaches remain at the level of participatory data collection. This narrative review examines citizen science approaches in participatory data generation, modelling and visualisation, and calls for truly participatory and co-creation approaches across all domains of pandemic preparedness and response. Further research is needed to identify approaches that optimally generate short-term and long-term value for communities participating in population health. Feasible, sustainable and contextualised citizen science approaches that meaningfully engage affected communities for the long-term will need to be inclusive of all populations and their cultures, comprehensive of all domains, digitally enabled and viewed as a key component to allow trust-building among the stakeholders. The impact of COVID-19 on people’s lives has created an opportune time to advance people’s agency in science, particularly in pandemic preparedness and response.
We anticipate that the intervention group will show significant changes in nutrition knowledge, attitudes, and practices; satisfaction with care; and …
Designing and Evaluating a Personalized, Human-Centered Dietary Decision Support System for Use Among People With Diabetes in an Indian Setting: Protocol for a Quasi-Experimental Study
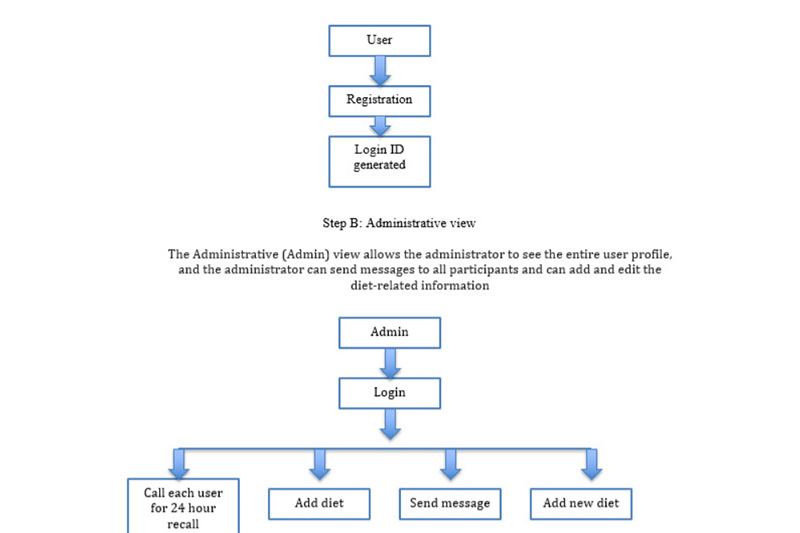
 We anticipate that the intervention group will show significant changes in nutrition knowledge, attitudes, and practices; satisfaction with care; and overall diabetes management. We also expect to see urban-rural differences across the groups. The uniqueness of our nutrient data capture process is demonstrated by its cultural and contextually relevant features-diet capture in both English and Hindi, diet conversion into caloric components, sustained diet data collection and participant adherence through telephone-linked care, and auto-generated reminders.
We anticipate that the intervention group will show significant changes in nutrition knowledge, attitudes, and practices; satisfaction with care; and overall diabetes management. We also expect to see urban-rural differences across the groups. The uniqueness of our nutrient data capture process is demonstrated by its cultural and contextually relevant features-diet capture in both English and Hindi, diet conversion into caloric components, sustained diet data collection and participant adherence through telephone-linked care, and auto-generated reminders.